Migraine and headaches

Virtual Reality: A New Era in Migraine Treatment
La réalité virtuelle propose une approche innovante pour soulager les migraines. Des études montrent son potentiel pour réduire la douleur grâce à des environnements immersifs.
Learn more
Foods to avoid during menstrual migraines
Menstrual migraine is a condition that affects many women but did you know that your diet could play a significant role in managing these migraines? Yes, you read that correctly . Certain foods can make your migraines worse, while others can help relieve them. Before diving into details, it's important to remember that every woman is unique. What may work for one person may not work for another. Listening to your body and keeping a food journal can be valuable tools in determining which foods trigger your migraines. It's not just about what we eat, but also when and how we eat. A healthy, balanced diet, combined with a healthy lifestyle, can make a big difference in pain management. In this article, we'll discuss foods to avoid during menstrual migraines, explain why certain foods are beneficial and why others are not , and provide tips for eating a diet that can help reduce symptoms. Overview of Foods to Avoid During Menstrual Migraines Explaining the impact of food on migraines Tips for a healthy diet and lifestyle Menstrual migraines: symptoms and causes Menstrual migraines are a common problem for many women. These dreaded headaches that usually occur before, during or after menstruation are often more severe than regular migraines. To understand why certain foods should be avoided during this time, it is crucial to first understand what causes these migraines. Symptoms of menstrual migraines Menstrual migraines primarily manifest as intense headaches, often felt on only one side of the head. They may be accompanied by nausea , vomiting and increased sensitivity to light or sound. The causes of menstrual migraines So why do these migraines occur during menstruation? The main cause is related to hormonal fluctuations that occur during the menstrual cycle . Specifically, a sudden drop in estrogen levels just before the start of your period can trigger a migraine. Additionally, menstrual cramps and stress associated with menstruation can also contribute to the onset of these migraines. The role of food Now you may be wondering: what does all this have to do with food? Well, certain foods can actually make migraine symptoms worse. For example, foods rich in tyramine, an amino acid that can trigger migraines, should be avoided. Likewise, foods that can cause bloating or water retention , such as those high in sodium, can increase blood pressure and make headaches worse. Conversely, other foods may be beneficial. Foods rich in magnesium, such as legumes, seeds and nuts, can help regulate estrogen levels and prevent migraines. Likewise, foods rich in omega-3 , such as fish and flaxseed , can help reduce inflammation and pain . It is important to note that every woman is different. What works for one may not work for another. That's why it's essential to work with a healthcare professional to develop a migraine management plan that meets your specific needs. The link between diet and menstrual migraines The link between diet and menstrual migraines is a subject that, although complex, deserves special attention. Indeed, certain foods can worsen menstrual migraine symptoms, while others can help relieve them. But why is this so? What makes a food good or bad for someone with menstrual migraines? Let's consider this more closely. Let's start by understanding the role of hormones in menstrual migraines. Hormonal changes that occur during the menstrual cycle can trigger migraines in some women. So foods that interact with these hormones, either by increasing their production or interfering with their function, can potentially exacerbate migraine symptoms. Also read: Migraine and female genital life Foods to Avoid Certain foods can trigger or worsen menstrual migraines. These foods include: Caffeine and alcohol: These two substances can cause fluctuations in blood pressure and blood sugar, which can trigger migraines. Additionally, caffeine may interfere with certain medications used to treat migraines. Processed foods: Highly processed foods often contain additives and preservatives that can trigger migraines. Additionally, they are often high in sodium, which can increase blood pressure. Foods rich in tyramine: Tyramine, a substance found in certain foods, can trigger migraines in some people. Foods high in tyramine include aged cheeses, sausages, and certain types of fish. Foods to favor So, what foods can help relieve menstrual migraines? These are mainly: Foods rich in magnesium: Magnesium can help prevent migraines by relaxing blood vessels. Foods rich in magnesium include green leafy vegetables, nuts and seeds, and legumes. Foods rich in omega-3: Omega-3, found in oily fish like salmon and tuna, can help reduce inflammation, which can help prevent migraines. Water: Dehydration is a common cause of migraines. Drinking enough water throughout the day can help prevent migraines. It is important to note that each person is unique and what works for one person may not work for another. So it's essential to experiment and find what works best for you. Additionally, it is always best to consult a healthcare professional before making any major changes to your diet, especially if you are taking medication for your migraines. Foods That Can Help Relieve Menstrual Migraines Menstrual migraines can be a real burden for many women. However, did you know that certain foods can help relieve those painful headaches ? It's crucial to be aware of what we put into our bodies, especially when suffering from migraines. Here is a list of foods that can help relieve your menstrual migraines. Foods rich in magnesium Magnesium is an essential mineral that has been linked to reducing migraines. Foods rich in magnesium include legumes, nuts, seeds, fish, and green leafy vegetables, such as spinach and kale. Healthy fats Healthy fats, like omega-3s, can help reduce inflammation, which is often a contributor to migraines. Sources of omega-3 include fatty fish such as salmon, mackerel and sardines, as well as nuts and seeds, such as flaxseed and walnuts. Foods rich in water Dehydration can often cause migraines, so eating foods that contain a lot of water can help prevent this problem. Cucumbers, melons, strawberries and peaches are good examples of water-rich foods. Whole grains Whole grains, like brown rice, quinoa, and oats, can help stabilize blood sugar levels, which can help prevent migraines. Additionally, they are an excellent source of fiber, which can help maintain a healthy digestive system . It's important to note that there is no miracle food that can eliminate menstrual migraines entirely. However, a balanced diet , combined with other healthy lifestyles, can help reduce the severity and frequency of these migraines. Ultimately, it's essential to listen to your body and take note of what seems to make your symptoms worse or better. Remember that every woman is different and what works for one person may not work for another. It is always best to consult a doctor or dietician before making any drastic changes to your diet. Foods rich in magnesium to fight menstrual migraines Menstrual migraine, an illness that affects a large number of women, can be reduced by making wise dietary choices. Among the most recommended nutrients to combat this type of migraine is magnesium. Why magnesium? Quite simply because it plays a crucial role in regulating the nervous system and helps control the body's reaction to pain. But where to find magnesium? Here is a list of foods that are naturally rich in it: Green leafy vegetables: such as spinach, kale and chard. Fruits: especially bananas, avocados and raspberries. Legumes: black beans, lentils and chickpeas are good sources. Nuts and seeds: Eat almonds, chia and flax seeds to increase your magnesium intake. Whole grains: such as quinoa, brown rice and oats. Dark chocolate: in moderate quantities, dark chocolate can be a valuable ally. However, it is important to note that although these foods are rich in magnesium, they are not a miracle solution for menstrual migraine. They must follow a balanced and varied diet, which also includes other essential nutrients. “Menstrual migraine is a complex condition that requires a comprehensive approach, including a balanced diet, a healthy lifestyle and, if necessary, appropriate medical treatment.” This is why, in addition to favoring foods rich in magnesium, it is crucial to consult a health professional to determine the best approach to adopt when dealing with your menstrual migraines. Foods rich in omega-3 to reduce the intensity of menstrual migraines Omega-3 fatty acids , known for their anti-inflammatory properties, may help reduce the intensity of menstrual migraines. These essential fatty acids, which cannot be produced by the body and must therefore be obtained through diet, have a beneficial effect on general health, including pain management. However, not all foods are created equal when it comes to their omega-3 content. Certain foods are particularly rich in these essential fatty acids and therefore may be more beneficial for those who suffer from menstrual migraines. Oily fish: Oily fish, such as salmon, mackerel and sardines, are among the richest sources of omega-3. Incorporating these fish into your diet can help reduce the inflammation and pain associated with menstrual migraines. Flaxseeds: Flaxseeds are an excellent source of omega-3 and can be easily added to various dishes, such as salads, smoothies and breakfast cereals. Nuts: Walnuts and almonds are rich in omega-3 and can be a great snack for those looking to increase their intake of these essential fatty acids. Nonetheless, it is important to note that the effectiveness of omega-3 fatty acids in reducing menstrual migraines may vary from person to person. For some people, a diet rich in omega-3 may help reduce the frequency and intensity of migraines, while for others it may not have a noticeable effect. It is therefore essential to take an individualized approach and consult a healthcare professional to discuss the best food choices to manage your menstrual migraines. Ultimately, while including omega-3 rich foods in the diet can help manage menstrual migraines, it is equally important to avoid certain foods that can trigger or worsen these headaches. Foods rich in vitamin B2 to prevent menstrual migraines Menstrual migraines, a discomfort that many women endure, can be greatly influenced by our diet. In fact, certain foods have the power to reduce or even prevent this pain. Among these, foods rich in vitamin B2 , or riboflavin, occupy a special place. But why then? Vitamin B2 plays a crucial role in the energy metabolism of our cells. Studies have shown that riboflavin can help reduce the frequency and intensity of migraines. In addition, it is known to improve the function of brain cells and protect nerves. So, what are these foods that are full of this precious vitamin B2? Let's take a look at this non-exhaustive list: Leafy green vegetables: These vegetables are an excellent source of vitamin B2. Think spinach, chard and broccoli. Eggs: In addition to being a source of protein, eggs are rich in vitamin B2. Dairy products: Milk, cheese and yogurt are sources of vitamin B2 that should not be neglected. Meat: Red meat and poultry are also good sources of vitamin B2. Whole grains: Not only are they rich in fiber, but they also contain vitamin B2. Note, however, that vitamin B2 needs may vary depending on individuals. It is therefore essential to adapt your diet according to your own needs. Additionally, although diet plays a key role, we must not forget the importance of a healthy lifestyle. Proper hydration, adequate sleep, and regular exercise can also help prevent menstrual migraines. The question therefore arises: does your diet contain enough vitamin B2 to prevent menstrual migraines? If this is not the case, do not hesitate to introduce the foods we have just mentioned into your daily diet. Your head will thank you! Processed foods to avoid to limit menstrual migraines Menstrual migraines can be unbearably intense, making daily tasks almost impossible to accomplish. One way to minimize these headaches is to carefully monitor your diet, especially avoiding certain processed foods . These foods, which seem so convenient and tasty, can actually help make migraines worse. For what? Because they often contain food additives, excess salt and preservatives that can trigger migraines. So, what processed foods should you avoid to limit menstrual migraines? Convenience foods: They often contain high levels of sodium, which can increase blood pressure and trigger migraines. Cold meats: They are high in nitrates and nitrites, which can dilate blood vessels and cause migraines. Fried foods: The trans fats they contain can cause inflammation that triggers migraines. Soft drinks: Their caffeine and sugar content can cause fluctuations in blood sugar, leading to migraines. It is important to note that every individual is different and sensitivity to these foods may vary. Plus, it's not just processed foods that can trigger migraines. Other factors, such as stress, lack of sleep and dehydration, may also play a role. It is therefore essential to take a holistic approach to managing your menstrual migraines. And remember: a balanced diet rich in fruits, vegetables, whole grains and lean proteins can make all the difference. So why not try replacing these processed foods with healthier alternatives? “Every step you take toward a healthier diet is a step toward better managing your menstrual migraines. Choose to favor fresh, unprocessed foods, and your body will thank you. » In short, if you suffer from menstrual migraines, it would be wise to review your diet and identify foods that could be triggers. By eliminating processed foods, you may see a significant reduction in the frequency and intensity of your migraines. Sugary foods to avoid to prevent menstrual migraines It's common to turn to sugary foods to relieve the stress and discomfort associated with menstruation. It may seem comforting in the moment, but did you know that consuming too much sugar can actually make menstrual migraines worse? Refined sugar, in particular, is known to trigger migraines due to its ability to cause blood sugar levels to spike, followed by sharp drops. These fluctuations can lead to severe headaches. Why are sugary foods harmful? Excessive sugar consumption can cause inflammation in the body, which can exacerbate menstrual migraines. Additionally, sugar can interfere with hormone levels in the body, which can also contribute to triggering headaches. So it would be wise to avoid these sugary foods during your period. Here is a list of these foods: Sweetened soft drinks Confectionery, such as candy and milk chocolate Pastries and cakes Sweet cereals Flavored yogurts It's not just about avoiding the obvious sweets. Some foods may contain hidden sugars. It is therefore important to read food labels carefully. If you're craving sugar, why not opt for healthier alternatives? Fresh fruit, for example, can satisfy your craving for something sweet while providing essential fiber, vitamins and minerals to your body. Or, try snacks made from nuts or seeds, which are high in protein and healthy fats to help you feel full longer and stabilize your blood sugar levels. Recommendations for a healthy and balanced diet in case of menstrual migraines When it comes to menstrual migraines, it is essential to understand that diet plays a determining role. Certain foods can trigger attacks, while others can help prevent or alleviate them. Focusing on a healthy, balanced diet can be a proactive approach to managing these migraines. But which foods to favor and which to avoid? Foods to favor It is first of all important to turn to foods that have a positive impact on health in general, and in particular on the management of menstrual migraines. Among them : Oily fish: rich in omega-3, fatty fish such as salmon, mackerel or sardines can help reduce inflammation and therefore reduce the intensity of migraines. Green leafy vegetables: They are an excellent source of magnesium, a mineral known to help prevent migraines. Nuts and seeds: they also provide a good dose of magnesium and can be easily integrated into the diet. Foods rich in vitamin B2: such as eggs, nuts and dairy products. A study has shown that high vitamin B2 consumption can reduce the frequency of migraines. Foods to Avoid Likewise, certain foods can triggermigraine attacks or worsen their symptoms. It is therefore preferable to avoid them, in particular: Processed foods: They often contain food additives, such as nitrites or glutamates, which can trigger migraines in some people. Caffeinated drinks: Caffeine can trigger migraines in some people. It is therefore preferable to moderate your consumption. Foods rich in histamine: such as mature cheeses, red wine and beer. Some people are sensitive to histamine and therefore may experience migraines after consuming these foods. Sugar and artificial sweeteners: They can cause spikes in blood sugar, which can trigger a migraine. In summary, eating a healthy, balanced diet can be an effective way to manage menstrual migraines. This involves favoring certain foods while avoiding others. It is important to note, however, that each person is unique and what works for one may not necessarily work for another. It may therefore be necessary to experiment and adjust your diet based on your specific needs and reactions to certain foods.
Learn more
Headaches and coffee: good or bad combination?
La caféine peut soulager ou aggraver les maux de tête selon les cas. Études et conseils pour mieux comprendre son impact sur les migraines et céphalées.
Learn more
Zavzpret (zavegepant), new Pfizer treatment for migraine
Zavzpret, à base de zavegepant, est un traitement de crise développé par Pfizer pour les migraines. Administré par spray nasal, il cible les récepteurs CGRP pour soulager rapidement la douleur. Cet article présente ses résultats cliniques, ses bénéfices, ses limites et son positionnement face aux autres gepants.
Learn more
Treatment of migraine during pregnancy and lactation
Cet article fait le point sur les traitements possibles de la migraine pendant la grossesse et l’allaitement.
Learn more
Catamenial menstrual migraines: definition and how to relieve them?
What is a catamenial migraine? Catamenial migraine is a migraine induced by the fluctuation of hormones during the menstrual cycle. They usually appear just before or just after menstruation. A distinction is made between pure menstrual migraine , which appears only at the time of menstruation; migraine induced by menstruation where in this specific case the patient also suffers from migraine at other times of the cycle. Catamenial migraine is therefore summarized as follows: Pure catamenial migraine : the patient suffers from a migraine once a month at the time of menstruation Induced catamenial migraine: the patient regularly suffers from migraine during the cycle, but mainly during menstruation Diagnosis of catamenial migraine To define catamenial migraines and establish an accurate diagnosis, attacks must occur two days before the onset of menstruation or up to three days after . Of course , the other diagnostic criteria for migraine must be respected : unilateral and throbbing headaches, which evolve by attack, associated with nausea or vomiting, sensitivity to light or noise and aggravated by physical activity. Catamenial migraine with aura Whether in pure menstrual migraine or in induced catamenial migraine, the patient may associate migraine auras . Migraine aura is a particular subtype of migraine in which the patient describes associated neurological disorders . Most often it is visual disturbances, such as the appearance of hatched lines in the visual field of small spots, we then speak of ophthalmic migraine . The migraine aura can, however, manifest itself through other symptoms such as speech disorders, motor or even sensory disorders. The migraine aura is the consequence of a massive excitation of neurons that spread like a wave or a wave on the surface of the cortex. This violent activation of certain neurons then causes the transient neurological symptoms that are associated with migraine aura . It was only in 2018 that catamenial migraine with aura was officially included among the list of headaches . To validate the diagnosis of catamenial migraine, it is necessary that the patient produces a migraine at least twice every three cycles . How to recognize a catamenial migraine? It is easy to recognize a catamenial migraine when it is said to be pure . That is to say when it occurs only during menstruation . However, when the patient has regular migraines, it is sometimes difficult to distinguish catamenial migraines from other migraines . Even if this point may seem futile, we will see later that the management of catamenial migraine can be different from traditional migraine. It is therefore important to note whether some migraines are specific to the menstrual cycle . For this, your doctor will advise you to follow a migraine diary . This diary must list all the information concerning your migraine attack, namely: the date and time of onset of the attack, the intensity of the attack, the possible triggering factor and the treatment taken. The analysis of this migraine diary will make it possible to make the link with the menstrual cycle of the woman and to see if migraines appear regularly near the day of the rules or if the migraines close to the menstruation are of an intensity more important than the others. Recognizing a catamenial migraine makes it possible to better understand the treatment of migraine, we will see later the fundamental role that hormones can play in these crises . It is however possible to modulate or limit the hormonal variation thanks to contraceptive pills for example. Recognizing catamenial migraine therefore makes it possible to precisely adapt a specific treatment. What Causes Catamenial Migraine The causes of catamenial migraine are essentially hormonal . It has been shown in several studies that menstrual migraines are the consequence of the significant variation in estrogen . Remember that migraine is an intolerance of the brain to change . Any significant variation can lead to the onset of a migraine attack . It is for this reason that thetriggering factors of migraine are so numerous (diet, stress, sleep, climatic environment, etc.). The sudden change in hormones can be considered by the brain as a change , and therefore participate in the triggering of a migraine attack. The role of estrogen and progesterone hormones The figure below shows how estrogen changes during the menstrual cycle . It is observed that during the phase of menstruation, the level of progesterone estrogen decreases considerably. If estrogen is mainly incriminated in the onset of migraine attacks, several studies tend to show that progesterone could also play a role . As part of a study on women's health were assessed whether the hormone level or variations differ between women with migraine compared to women in a control group . In order to explore the hypothesis that women with migraine have distinct hormonal profiles , they compared daily hormone peaks and levels between all of these women across the menstrual cycle. Interestingly, in this study, there was no significant difference between migraineurs and controls in estrogen peaks or average daily levels. In contrast, there is a significant difference between the two groups in the rate of estrogen decline , particularly at the end of the luteal phase , just after ovulation. In addition, in migraineurs, the rate of estrogen decline does not distinguish between cycles with and without acute headache. This finding suggests that a neuroendocrine vulnerability characterizes female migraineurs and may facilitate the onset of the migraine attack . Interestingly, these pathophysiological considerations regarding migraineurs versus controls might also underlie the more specific condition of menstrual migraineurs. On the other hand, no clear relationship between progesterone fluctuations during the menstrual cycle and migraine attacks was found in this study. Estrogens also implicated in endometriosis The variation of ovarian hormones is also implicated in the modulation of chronic pain and particularly in endometriosis. Several studies have shown the protective effect of estrogen against the onset of pain. They have natural anti-inflammatory activity . It is also for this reason that their decrease during the menstruation phase can facilitate the appearance of inflammation and therefore of acne or endometriosis, etc. In the case of migraine, the variation in estrogens can have a double impact : on the one hand, resulting in a significant variation for the brain and therefore being considered as a triggering factor for migraine , and on the other hand, the reduction in their rate. facilitates the onset of inflammation and therefore promotes the intensity of migraines. Estrogens influence prostaglandins in catamenial migraine It has been shown that the decrease in estrogen is likely to lead to a massive release of prostaglandins . Prostaglandins are immune system proteins that promote inflammation . In women, they are massively released during the luteal phase of the cycle, that is to say just after ovulation. During the period of menstruation, the amount of estrogen is at its lowest and therefore the release of prostaglandins is important, which promotes the appearance of inflammation and therefore migraines . The role of CGRP and neuropeptides in menstrual migraine The massive release of prostaglandins linked to the drop in estrogen levels will cause the massive release of neuropeptides . Among them we can note substance P or the gene linked to the calcitonin peptide (CGRP). These neuropeptides are involved in triggering migraine attacks and maintaining pain . They are released by a special system called the trigeminovascular system . This system is involved in the innervation of the meninges which is the envelope of the brain and its blood vessels . During a migraine attack, this system will massively release these neuropeptides which will cause strong inflammation and at the same time vasodilatation , that is to say a significant dilation of the blood vessels. This inflammatory reaction on the meninges is at the origin of the pain felt by the patient . Hormonal fluctuations in women have been shown to directly influence the amount of CGRP contained in the trigeminovascular systems. A study has also shown that the level of CGRP found in blood plasma is significantly higher in women than in men . This confirms the correlation with the menstrual cycle and may potentially explain why women are more prone to migraines than men . How many women suffer from catamenial migraines? Several studies have attempted to quantify the number of female migraine sufferers with catamenial migraine . It is known that 15 to 20% of the population suffers from migraine, among these patients two thirds are women . A recent study established in Norway on 5000 female migraine sufferers showed that 6% of women suffered from catamenial migraine. 6.1% suffered from catamenial migraine without aura and 0.6% with aura. If we consider all women, the prevalence of catamenial migraine would be around 1%. Menstrual migraine during a woman's lifetime During pregnancy The relationship between the menstrual cycle and catamenial migraines may change over the course of a woman's reproductive life . A study reports that catamenial migraines appear after the age of 30 preferably. During pregnancies , women who suffer from catamenial migraines have reported much more intense migraines at the beginning of this one. During the postpartum this observation is identical. As in the majority of women, the second and third trimester phase of pregnancy is often a sign of a significant reduction in the frequency of migraine attacks . This is hormonal stability with a high dose of estrogen that protects the woman from the appearance of new crises. During menopause Significant fluctuations in estrogen levels occur during perimenopause , which is when menopause begins to set in. These fluctuations lead to a significant decrease in estrogen levels . As a result, the majority of women with migraine report seeing an intensification of migraine attacks during this period. Fortunately, when menopause sets in, hormonal stability usually leads to a decrease in the frequency of seizures . How to treat catamenial migraine? Crisis treatment and basic treatment Generally catamenial migraine attacks are more difficult to respond to usual migraine attack treatments . Additionally, there is currently no specific treatment for catamenial migraine . However, the intensity of the pain requires the implementation of an effective treatment. For this reason, treatment for seizures will always be prescribed to the patient. Triptans are the most common treatment. It will also be necessary to add a preventive treatment, which is also called basic treatment or prophylactic treatment of migraine . Unlike the treatment of seizures which is taken to stop it when it happens, the background treatment aims to gradually reduce the frequency of seizures . Generally a basic treatment must be taken every day and is evaluated over three to six months. Studies have shown that the combination of a triptan and a nonsteroidal anti-inflammatory drug would be much more effective in the case of catamenial migraines. The addition of anti-inflammatories then compensates for the anti-inflammatory effect of estrogens. The pill and contraceptives The use of hormonal contraceptives such as the pill or certain IUDs and a plan can play on the fluctuation of hormones . For this reason it is essential that the patient consults her doctor or her gynecologist in order to prescribe a contraceptive that will stabilize estrogen and hormonal variations as much as possible. This phase of the treatment sometimes requires several months of adaptation and it is very rare to succeed on the first try. However, it is important to persevere, because the benefit can be considerable . The natural treatment for catamenial migraine There are also natural treatments that help regulate hormone levels in patients. We can cite a few medicinal plants such as Siberian rhubarb , black cohosh or chaste tree . There are very few clinical studies that have proven the effectiveness of these plants, however the effectiveness is traditionally recognized and accepted in the European Pharmacopoeia. Other natural migraine treatments like MIGSPRAY use polymeric plant extracts to target CGRP at the nasal level. These plants and can be associated with your basic treatments and crises.
Learn more
La migraine, une maladie complexe
Chaque jour, des millions de personnes ressentent une douleur lancinante, sourde ou intense, qui frappe un côté de la tête ou les deux. Ce n’est pas un simple mal de tête : c’est une crise migraineuse.
Une maladie neurologique complexe, souvent chronique, qui peut durer des heures, voire des jours, et bouleverser une vie. Lumière, bruit, odeur, tout devient insupportable.
Certains patients sont touchés dès l’enfance, d’autres voient apparaître les premiers symptômes à l’âge adulte, souvent sans comprendre leur origine.
Plusieurs types de migraines
Il existe plusieurs types de migraines, aux origines variées :
vasculaires, neuronales ou hormonales. Les douleurs peuvent s’accompagner de nausées,
de vomissements, de troubles visuels, voire parfois de paralysies
transitoires. Chaque forme a ses propres déclencheurs, une intensité
variable et une fréquence différente.

Des causes variables
Pour de nombreuses personnes, le diagnostic est tardif, les examens se multiplient, et les traitements s’enchaînent sans réel succès.
Les causes et symptômes sont nombreux, variés, parfois atypiques : les
connaître, c’est la première étape pour soulager efficacement la migraine.
Mais les recherches avancent. Grâce aux progrès sur la physiopathologie, les neuropeptides, le cortex, le tronc cérébral ou l’inflammation vasculaire, de nouveaux traitements apparaissent.
Comprendre la migraine, c’est reprendre le contrôle sur sa santé, sur son corps, sur sa vie.
Qu'est-ce que la migraine ? Définition
La migraine est une maladie neurologique chronique marquée par des crises de céphalées récurrentes, modérées à sévères, souvent ressenties d’un seul côté de la tête. Bien plus qu’un simple mal de tête, chaque crise migraineuse peut durer de 4 à 72 heures et s’aggraver avec le moindre effort physique.
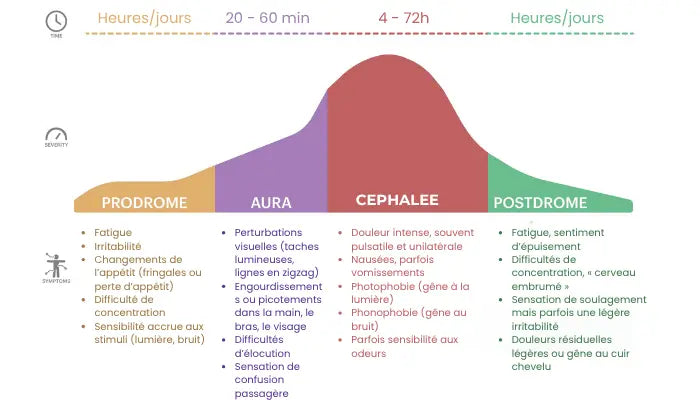
Les phases de la migraine
Ce schéma représente les 4 phases de la migraine : les prodromes, l'aura, la céphalée et les postdromes.

Conférence sur la migraine
Visionnez le replay de cette conférence animée par le Dr Shrivastava lors de la journée de la douleur.
Symptômes associés
Tableau comparatif des céphalées les plus courantes :
À retenir : la migraine est d’origine neurologique, liée à une dysfonction transitoire du cerveau, impliquant les neurones, les vaisseaux sanguins et la libération de neuropeptides comme le CGRP. Ce n’est ni une maladie vasculaire, ni simplement hormonale, ni psychologique.
Durée et type de douleur :
| Type de céphalée | Durée | Douleur |
|---|---|---|
| Migraine | 4 à 72 h | Pulsatile, souvent unilatérale |
| Céphalée de tension | 30 min à 7 jours | Sensation de serrement, bilatérale |
| Algie vasculaire de la face | 15 min à 3 h | Brûlure intense autour de l’œil |
Symptômes associés et intensité :
| Type de céphalée | Symptômes associés | Intensité |
|---|---|---|
| Migraine | Nausées, vomissements, photophobie, phonophobie | Modérée à sévère |
| Céphalée de tension | Fatigue, tension cervicale, pas de nausée | Légère à modérée |
| Algie vasculaire de la face | Larmoiement, nez bouché, agitation | Très sévère |

Une pathologie qui bouleverse la vie
La migraine est invisible, mais son retentissement est bien réel. Pour ceux qui en souffrent régulièrement, elle peut affecter toutes les dimensions de la vie quotidienne. Elle touche environ 15 % de la population mondiale, et constitue l’une des principales causes d’années vécues avec handicap selon l’OMS.
La migraine n’est donc pas une simple gêne ponctuelle, mais bien une maladie chronique, avec des mécanismes complexes et des manifestations multiples. Mieux la comprendre, c’est le premier pas vers un diagnostic plus rapide, un traitement adapté et une meilleure qualité de vie.
Conséquences courantes de la migraine sur la vie des patients
L'impact sociale de la migraine
Cette étude, menée avec l’association La Voix des Migraineux, donne la parole à 683 patients migraineux en France. Elle révèle :
- Un parcours de soins difficile : 7,5 ans en moyenne pour obtenir un diagnostic.
- Un handicap sévère : 96 % des participants ont un score HIT-6 élevé, et 70,7 % un score MIDAS indiquant une forte incapacité.
- Un impact professionnel et social majeur : 36 % décrivent leur parcours comme un "parcours du combattant", et plus de la moitié ne se sentent ni écoutés ni soutenus par les professionnels de santé.
- Un besoin criant d’amélioration du système de soins : retards de traitement, effets secondaires mal pris en charge, manque d’accès aux spécialistes.
Un plafond de verre
- Chez l’enfant : absences répétées à l’école, difficultés de concentration, anxiété
- Chez l’adulte actif : arrêts de travail fréquents, perte de productivité
- Chez les femmes : crises liées au cycle menstruel, influence hormonale marquée
- Sur le bien-être psychologique : repli sur soi, peur de la prochaine crise, incompréhension de l’entourage
- Dans la vie sociale : isolement, annulations de dernière minute, perte de spontanéité
Chaque personne migraineuse a un profil différent :
- Certaines font une crise par an, d’autres plusieurs par semaine
- La douleur peut durer 2 heures ou 3 jours
- Les symptômes associés varient : visuels, digestifs, neurologiques, etc.
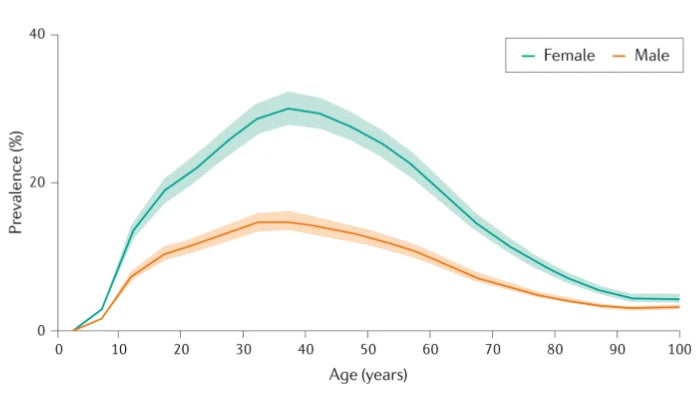
Le graphique suivant montre l'évolution de la prévalence de la migraine selon l'âge.
De plus en plus de patients migraineux
Cette analyse des données du Global Burden of Disease montre que :
- La prévalence mondiale de la migraine a augmenté de 58 % entre 1990 et 2021, atteignant 1,16 milliard de personnes.
- La migraine est la 2e cause mondiale de handicap (en années vécues avec une incapacité).
- Les adolescents et les hommes voient une croissance rapide de la prévalence.
- Les projections indiquent une hausse continue jusqu’en 2050, avec des implications majeures pour les politiques de santé publique.
Rejoignez la communauté ChèreMigraine
Entrez votre e-mail pour rejoindre ChèreMigraine et recevoir votre premier cadeau
Une communauté de patients migraineux
Vous souffrez de migraines ? Vous n’êtes pas seul.e.
Des milliers de patients comme vous ont déjà rejoint ChèreMigraine, la communauté dédiée à celles et ceux qui veulent mieux comprendre, mieux gérer… et mieux vivre avec leurs migraines.
En vous inscrivant avec votre e-mail, vous recevrez :
- astuces concrètes pour soulager les crises,
- conseils de spécialistes,
- cadeaux exclusifs, comme notre Cahier des Migraines
- l'actualités scientifiques sur la migraine, directement dans votre boîte mail.
Vous pouvez aussi nous retrouver sur Instagram ( @Chèremigraine ) pour échanger avec la communauté, partager vos expériences et rester informé.e au quotidien.
Identifier les différents types de migraines
La migraine n’a pas une seule et unique présentation. Derrière ce mot se cache une grande diversité de formes cliniques, avec des durées, des symptômes et des intensités très variables. Il est essentiel de comprendre que toutes les migraines ne se ressemblent pas : bien identifier le type de migraine dont on souffre est une étape clé vers un diagnostic précis et un traitement adapté.
Pour aller plus loin et découvrir davantage les différentes formes de migraine (avec ou sans aura, migraine ophtalmique, hémiplégique, etc.), explorez notre article : Les types de migraines.

Migraine sans aura
C’est la forme de migraine la plus fréquente : elle représente environ 75 % des cas.
Elle se manifeste par :
- Une douleur pulsatile, souvent localisée d’un seul côté de la tête (mais parfois bilatérale)
- Une intensité modérée à sévère
- Une durée de 4 à 72 heures
- Des symptômes associés :
nausées, vomissements,
photophobie, phonophobie...
Elle survient sans signe annonciateur évident (comme une aura), bien que certains patients puissent ressentir une phase de prodrome avant la douleur.

Migraine avec aura
La migraine avec aura concerne environ 20 à 25 % des personnes migraineuses. Elle se caractérise par l’apparition de symptômes neurologiques transitoires qui précèdent (ou accompagnent) la douleur.
Les auras peuvent être :
- Visuelles (les plus fréquentes) : points scintillants, lignes en zigzag, taches sombres ou floues
- Sensorielles : picotements, engourdissement d’un bras ou du visage
- Motrices (plus rares) : sensation de faiblesse musculaire ou troubles de la parole
Ces symptômes apparaissent progressivement en 5 à 60 minutes, durent généralement moins d’une heure, et disparaissent totalement. La céphalée peut survenir immédiatement après, ou être différée de quelques heures.

Formes rares ou atypiques
Certaines migraines présentent des manifestations inhabituelles ou concernent des populations spécifiques.
- Migraine ophtalmique : se manifeste par des troubles visuels importants
- Migraine hémiplégique : très rare, elle provoque une faiblesse temporaire d’un côté du corps, imitant un AVC.
- Migraine vestibulaire : caractérisée par des vertiges récurrents (avec ou sans douleur), troubles de l’équilibre et nausées intenses.
- Migraine abdominale : typique de l’enfant, elle provoque des douleurs abdominales intenses par crises, sans douleur à la tête.
- Migraine cataméniale : liée au cycle menstruel, elle survient dans les jours précédant les règles, souvent plus longue et résistante aux traitements habituels.

La migraine chronique
La migraine chronique est une forme sévère de migraine, définie par :
- ≥ 15 jours de céphalées par mois , dont au moins 8 jours avec critères de migraine
- Une durée supérieure à 3 mois
- Un impact majeur sur la qualité de vie, la productivité et le moral
- Une association fréquente à des comorbidités : anxiété, dépression, troubles du sommeil
- Un risque accru d’abus médicamenteux et de passage en migraine réfractaire
Elle nécessite une prise en charge médicale spécialisée, avec des traitements de fond adaptés et un suivi régulier pour espérer réduire la fréquence des crises.

Données épidémiologiques
La migraine est l’une des affections neurologiques les plus répandues, bien plus qu’on ne le pense. Selon l’Organisation mondiale de la santé (OMS), elle touche environ 1 personne sur 7 dans le monde, soit près de 1 milliard d’individus. Ce chiffre impressionnant place la migraine au même rang que d'autres grandes maladies chroniques comme le diabète ou l'asthme mais avec une reconnaissance publique et médicale encore largement insuffisante.
Elle ne se limite pas à un continent ou à une culture. La migraine concerne tous les groupes ethniques, tous les niveaux socio-économiques, et elle est présente dans toutes les zones géographiques. Bien que les conditions de diagnostic et de prise en charge varient selon les pays, le fardeau de la maladie reste global.
Poids socio-économique
La migraine est non seulement fréquente, mais elle est aussi l’une des principales causes de perte de qualité de vie dans le monde. Selon l’étude Global Burden of Disease publiée dans The Lancet, la migraine représente la 2e cause mondiale d’années vécues avec un handicap (YLD) chez les moins de 50 ans, toutes maladies confondues.
Ce retentissement fonctionnel massif s’explique par :
- La fréquence des crises, souvent imprévisibles, qui empêchent toute planification d'activité
- La sévérité des symptômes : douleurs, troubles sensoriels, nausées invalidantes
- L’impact sur la productivité : baisse de concentration, absentéisme répété, fatigue persistante
Ce fardeau invisible génère des coûts importants :
- Arrêts de travail fréquents dans les périodes de crise
- Dépenses de santé répétées : consultations, examens, traitements parfois inefficaces
- Errance diagnostique : patients mal orientés, explorations inutiles, retards de prise en charge
- Hospitalisations ponctuelles, notamment en cas de migraine chronique ou résistante
Et pourtant, dans de nombreux pays, la migraine reste sous-diagnostiquée, sous-traitée et sous-financée. Elle est encore trop souvent perçue comme une gêne mineure, alors qu’elle constitue une véritable maladie chronique handicapante.
Les personnes atteintes de migraine chronique (plus de 15 jours de migraine par mois) sont particulièrement exposées à une dégradation de leur qualité de vie, mais aussi à des comorbidités (anxiété, dépression, troubles du sommeil). La migraine ne s’exprime pas de la même façon chez chacun. Certains patients ne font qu’une crise par an, d’autres peuvent en avoir plusieurs par semaine. Cette variabilité complique sa reconnaissance et sa prise en charge.
Face à cette diversité de situations, il est essentiel d’adopter une approche personnalisée. Pour découvrir des solutions concrètes et des conseils pratiques au quotidien, consultez notre article dédié : Comment soulager la migraine ?

Le rôle du système nerveux central
La migraine ne naît pas dans les artères… mais bien dans le cerveau. Le cerveau migraineux devient hypersensible à des stimuli bénins (lumière, bruit, odeur), en raison d’une activation anormale de circuits neuronaux : c’est la sensibilisation centrale.
Zones impliquées dans le déclenchement et le maintien de la migraine :
Le cortex cérébral
Le cortex cérébral, en particulier dans les migraines avec aura, présente une hyperactivité soudaine suivie d’une onde de dépression électrique appelée dépression corticale envahissante. Ce phénomène entraîne des troubles visuels, sensoriels ou moteurs en fonction des zones touchées, avant même que la douleur n’apparaisse.
Le tronc cérébral
Le tronc cérébral, en particulier les noyaux du nerf trijumeau, agit comme un centre de transmission de la douleur. C’est lui qui relaie les signaux nociceptifs vers le cerveau et active une réponse inflammatoire dans les méninges, les fines membranes qui entourent le cerveau.
L’hypothalamus
L’hypothalamus est souvent activé dans les heures précédant la crise. Cette structure régule de nombreuses fonctions biologiques :
sommeil, appétit, hormones,
stress… autant de facteurs déclenchants identifiés dans la migraine. Certains patients ressentent d’ailleurs des signes avant-coureurs (envies alimentaires, irritabilité, bâillements) plusieurs heures avant la douleur : c’est la phase de prodrome, directement liée à l’hypothalamus.
Le nerf trijumeau
Le nerf trijumeau, qui innerve le visage et une grande partie du crâne, joue un rôle central dans la génération de la douleur migraineuse. Lorsqu’il est activé, il libère des substances inflammatoires dans les méninges, contribuant à l’amplification de la douleur.

Inflammation neurovasculaire et neurotransmetteurs
Le rôle des vaisseaux sanguins ne disparaît pas pour autant. Lors d’une crise, on observe une dilatation des vaisseaux méningés, c’est-à-dire les vaisseaux situés dans les membranes entourant le cerveau. Cette dilatation n’est pas la cause unique de la douleur, mais elle contribue à une
inflammation neurogénique locale.
Cette inflammation est alimentée par la libération de plusieurs
neurotransmetteurs et neuropeptides :
Le CGRP
Le CGRP (Calcitonin Gene-Related Peptide) est aujourd’hui au cœur de la recherche migraineuse. Il est libéré par les neurones du nerf trijumeau et provoque à la fois vasodilatation, inflammation
et transmission de la douleur. Les nouveaux traitements anti-CGRP ciblent directement ce mécanisme.
La sérotonine
La sérotonine (5-HT) joue un rôle ambivalent. En baisse avant la crise, elle pourrait être un déclencheur indirect. Les triptans, traitements classiques de la crise, agissent en partie sur les récepteurs à sérotonine.
La dopamine
La dopamine, impliquée dans la régulation de l’humeur, de la motivation et du système digestif, peut expliquer certains
symptômes associés à la migraine (nausées, troubles gastro-intestinaux, fatigue intense).
La substance P
La substance P et le glutamate
participent à l’entretien de l’inflammation et à l’excitation prolongée des neurones de la douleur.

Terrain génétique et hypersensibilité neuronale
Pourquoi certaines personnes sont-elles plus sujettes à la migraine que d’autres ? La réponse se trouve en partie dans les gènes. Certaines mutations ont été identifiées dans les formes familiales rares, comme la migraine hémiplégique. Ces mutations affectent le transport des ions (calcium, sodium) à travers les membranes neuronales, modifiant la réactivité des neurones.
Mais même dans les formes non héréditaires, la prédisposition familiale est très fréquente : plus de 70 % des patients migraineux ont un parent également touché.
Cette susceptibilité génétique s’exprime souvent par une hypersensibilité neuronale :
- Les stimuli sensoriels (lumière vive, bruits, odeurs) sont perçus comme agressifs
- Le cerveau réagit de façon exagérée au manque de sommeil, au stress, ou à certains aliments
- L’excitation neuronale n’est pas correctement modulée, ce qui facilite le déclenchement des crises
Ce terrain particulier explique la variabilité d’une personne à l’autre, mais aussi d’une crise à l’autre. Il souligne l’importance d’une approche personnalisée dans le diagnostic et la prise en charge.
Causes, facteurs et risques déclencheurs
La migraine ne survient pas au hasard. Si ses mécanismes neurologiques sont aujourd’hui mieux compris , ses causes profondes restent encore partiellement élucidées. On sait toutefois qu’elle résulte de facteurs multiples: génétiques, hormonaux, environnementaux et sensoriels. Ces éléments influencent à la fois la prédisposition à souffrir de migraine et la fréquence des crises.
Pour aller plus loin, découvrez notre article dédié aux causes et symptômes de la migraine, afin de mieux reconnaître les signaux du corps et comprendre les mécanismes en jeu.










Les 4 phases de la crise migraineuse
Une crise migraineuse ne commence pas et ne se termine pas avec la douleur. Elle se décompose souvent en plusieurs phases successives, qui peuvent s’étaler sur plusieurs heures, voire plusieurs jours.
Les 4 grandes phases :
Le prodrome (quelques heures à deux jours avant la crise) :
- Signes précoces : bâillements, irritabilité, fringales, difficulté à se concentrer
- Cette phase est souvent sous-estimée, mais peut aider à anticiper la crise
L’aura (chez 20 à 25 % des patients) :
- Troubles visuels (scintillements, flous, lignes en zigzag), troubles sensoriels ou moteurs
- Dure de 5 à 60 minutes, précède généralement la douleur
La phase douloureuse :
- Douleur intense, unilatérale, pulsatile
- Symptômes associés (nausées, photophobie, phonophobie...)
- Peut durer de 4 à 72 heures si non traitée
Le postdrome (phase de récupération) :
- Sensation de fatigue extrême, confusion, corps « vidé »
- Peut durer 24 à 48 heures après la disparition de la douleur
Comprendre ces phases permet de mieux anticiper les crises et d’adapter le traitement dès les premiers signes.

Quand consulter un spécialiste ?
La migraine peut souvent être diagnostiquée par un médecin généraliste, mais certaines situations nécessitent l’avis d’un neurologue ou d’un centre spécialisé dans les céphalées.
Voici quelques situations où une consultation spécialisée est recommandée :
- Douleur inhabituelle ou brutale, surtout si elle apparaît soudainement (« coup de tonnerre »)
- Aggravation rapide de la fréquence ou de l’intensité des crises
- Anomalies neurologiques inhabituelles : perte de vision, trouble de la parole, paralysie
- Échec des traitements de crise classiques ou suspicion de migraine chronique
Il est important de ne pas banaliser une migraine qui change de forme, s’intensifie, ou s’accompagne de signes atypiques. Dans certains cas, ces symptômes peuvent révéler une pathologie plus grave (AVC, tumeur, méningite), d’où l’importance de ne pas retarder le diagnostic.
À noter : une migraine stable depuis plusieurs années, avec symptômes classiques, ne nécessite pas systématiquement d’imagerie cérébrale.

L’importance du suivi
Une fois le diagnostic posé, il est essentiel de mettre en place un suivi régulier, même si les crises sont peu fréquentes. La migraine est une maladie évolutive : sa fréquence, son intensité et ses déclencheurs peuvent changer avec le temps.
Voici les éléments clés d’un bon suivi :
- Tenue d’un journal de crise : fréquence, durée, symptômes, déclencheurs, réponse au traitement
- Consultations régulières : pour ajuster le traitement, évaluer le retentissement, repérer un passage à la migraine chronique
- Évaluation du retentissement sur la qualité de vie : échelle MIDAS, HIT-6, ou questionnaires spécialisés
- Adaptation du traitement de fond en fonction de l’évolution : un traitement efficace au début peut ne plus l’être après quelques mois
Un bon suivi permet aussi d’anticiper les complications, comme la surconsommation médicamenteuse (cause fréquente de céphalée chronique) ou les comorbidités psychologiques (anxiété, dépression).

Traitements de crise et de fond
Il n’existe pas de solution universelle pour soulager la migraine : les traitements doivent être personnalisés.
Traitements de la crise
Les traitements de crise ont pour objectif de stopper la douleur le plus rapidement possible, et de limiter les symptômes associés (nausées, vomissements, photophobie…).
Médicaments utilisés :
- AINS (anti-inflammatoires non stéroïdiens)
- Triptans : médicaments spécifiques de la migraine
- Antiémétiques
Alternatives complémentaires :
- Huiles essentielles : la menthe poivrée ou la lavande vraie
- Repos dans le noir et le silence
- Techniques de relaxation
Traitements de fond
Lorsque les crises deviennent trop fréquentes (plus de 4 jours par mois) ou très invalidantes, un traitement de fond peut être proposé. Son objectif : diminuer la fréquence, l’intensité et la durée des crises, voire les faire disparaître.
Médicaments préventifs classiques :
- Bêtabloquants (propranolol, métoprolol)
- Antiépileptiques (topiramate, valproate)
- Antidépresseurs tricycliques (amitriptyline)
- Anticorps anti-CGRP (erenumab, galcanezumab, fremanezumab)
| Profil migraineux | Caractéristiques | Traitement recommandé |
|---|---|---|
| Migraine épisodique sans aura | Crises peu fréquentes, douleur unilatérale pulsatile, nausées | AINS, triptans au besoin, hygiène de vie |
| Migraine avec aura | Troubles visuels ou sensoriels avant la douleur | Triptans dès l’aura, traitement de fond si récurrence |
| Migraine cataméniale | Crises liées aux menstruations, souvent résistantes | Triptans, anti-inflammatoires, traitement hormonal ciblé |
| Migraine chronique | ≥ 15 jours de maux de tête/mois dont ≥ 8 jours de migraine | Traitement de fond (anti-CGRP, bêtabloquants, TENS) |
| Migraine résistante ou médicamenteuse | Échec des traitements classiques, abus médicamenteux | Sevrage, centre anti-douleur, alternatives non médicamenteuses |
Mieux vivre avec la migraine au quotidien
La migraine ne se soigne pas seulement par des médicaments. Elle se gère aussi au quotidien par l’observation, la prévention et l’adaptation. Comprendre sa maladie, identifier ses déclencheurs et ajuster son environnement permettent souvent de réduire la fréquence des crises et de retrouver une meilleure qualité de vie. Il ne s’agit pas simplement d’éviter ce qui fait mal, mais d’apprendre à composer avec une sensibilité neurologique particulière.
Éviter les déclencheurs
Identifier les éléments qui précèdent ou favorisent les crises est un point clé dans la gestion de la migraine. Ce n’est pas une démarche standard : chaque patient est unique.
Trois piliers à surveiller :
- Routine de sommeil : se coucher et se lever à heure fixe, éviter les variations brutales (week-ends, décalages horaires), limiter les écrans en soirée.
- Gestion du stress : relaxation, sophrologie, activité physique douce, cohérence cardiaque. Le stress est un des facteurs les plus fréquemment retrouvés avant une crise.
- Hygiène de vie globale : alimentation régulière, bonne hydratation, suppression des excès (café, sucre, alcool), pauses fréquentes en cas de travail sur écran.
Tenir un journal de crise permet de croiser les déclencheurs potentiels (nourriture, émotions, météo...) et d’identifier les profils de risque.
Adapter son environnement
L’environnement sensoriel joue un rôle majeur dans le déclenchement ou l’aggravation d’une migraine. Adapter son cadre de vie peut grandement limiter les agressions visuelles, sonores ou olfactives.
Quelques ajustements simples :
- Lumière : privilégier la lumière naturelle tamisée, utiliser des filtres pour écrans, éviter les éclairages LED trop blancs ou clignotants.
- Bruit : écouteurs avec réduction de bruit passive, zones calmes au travail ou à l’école, pauses sensorielles régulières.
- Odeurs : éviter les parfums forts, aérer régulièrement les pièces, choisir des produits d’entretien neutres.
- Poste de travail : écran à bonne hauteur, siège ergonomique, pauses oculaires toutes les 20 minutes.
Ces mesures réduisent la charge sensorielle subie par le cerveau, en particulier lors des phases prodromiques où il devient plus vulnérable.
En parler autour de soi
La migraine est souvent invisible. Pourtant, elle a des répercussions sociales, scolaires et professionnelles majeures. En parler est essentiel pour obtenir du soutien et adapter son quotidien sans culpabilité.
Pourquoi communiquer sur sa migraine ?
- En milieu professionnel : aménagements possibles (horaires flexibles, télétravail, pauses supplémentaires, poste adapté)
- En milieu scolaire : meilleure tolérance des absences, adaptation des examens ou des rythmes d’apprentissage
- Dans le cercle familial : compréhension des crises, réduction du stress relationnel, meilleure gestion des responsabilités
L’acceptation de la migraine comme une vraie pathologie neurologique est une étape importante pour le patient. Ce n’est pas une faiblesse, ni un simple mal de tête, mais une condition chronique avec un retentissement réel sur la qualité de vie .
Des associations comme La Voix des Migraineux proposent des ressources pour expliquer la migraine à ses proches, à ses collègues ou à ses enseignants.
Pour aller plus loin, explorez notre article : Comment soulager la migraine ?

Ce que la migraine révèle de notre cerveau
Et si la migraine n'était pas uniquement une pathologie à éliminer, mais également une manifestation des stratégies de régulation ? Certains neurologues proposent une lecture évolutive de la migraine. Le cerveau migraineux serait en réalité un cerveau hyper-réactif, conçu pour détecter très tôt les menaces : surcharge sensorielle, fatigue extrême, danger environnemental. La crise migraineuse serait alors une réponse de protection.
En cas de surcharge le cerveau migraineux déclencherait une crise pour interrompre brutalement l’activité neuronale excessive. Ce processus, impliquant notamment la dépression corticale envahissante ou la libération de neuropeptides comme le CGRP, serait une forme extrême de protection des circuits supérieurs.
Un modèle pour mieux comprendre la douleur chronique :
- Mieux comprendre les mécanismes de chronicisation de la douleur
- Identifier les structures cérébrales impliquées dans la modulation de la douleur
- Explorer de nouvelles cibles thérapeutiques comme les traitements anti-CGRP, la stimulation magnétique transcrânienne, ou la modulation des réseaux neuronaux impliqués dans la douleur



Your cart
0
Your cart is currently empty.
Vous ne savez pas par où commencer ? Essayez ces collections :

- Choosing a selection results in a full page refresh.
- Opens in a new window.